dr. Székely Margit
physician specializing in physical rehabilitation
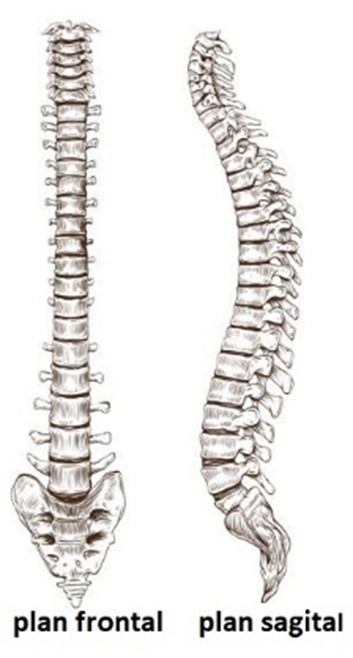
The spine is the central component of the human musculoskeletal system. It must ensure an optimal balance between stability and mobility so that it can support the body’s weight while allowing for an adequate range of motion necessary for efficient biomechanical function. As an adaptation to the upright posture, the spine has four physiological curves in the sagittal plane that increase its strength, allow for shock absorption during locomotion, and facilitate its mobility. The normal spine is straight in the frontal plane.
Scoliosis is the most common disorder of spinal alignment in the frontal plane. It is an abnormal lateral curvature of the spine and is one of the most common conditions in children and adolescents. It can be classified into two main types: functional and structural.
In functional, nonstructural scoliosis, the anatomy of the vertebrae and discs is normal; only the alignment in the frontal plane is disrupted. The lateral deviation of the spine is completely reducible, both clinically and radiographically, in the supine position.
In structural scoliosis, the vertebrae exhibit structural changes (rotations, wedge-shaped deformities). The lateral deviation of the spine is clinically and radiologically irreducible in the supine position. Idiopathic scoliosis is the most common form of structural scoliosis. The lateral deviation of the spine occurs in a healthy child, with no exact cause being identifiable.
From an etiological perspective, functional scoliosis includes scoliotic postures (without an obvious cause), reducible scoliotic curves (which are usually antalgic postures associated with spinal conditions), and compensatory curves resulting from certain conditions (e.g., lower limb length discrepancy). Structural scoliosis is most often idiopathic, with no known cause.
For the diagnosis of scoliosis, the most important step is the clinical examination, which allows for the identification of the characteristic signs of spinal curvature. This examination must be performed with the patient undressed, wearing only briefs. The entire body must be examined while the patient is standing, viewed from the front, in profile, and from the back. Attention should be paid to the symmetry of the shoulders and shoulder blades; the symmetry of the waist triangles formed between the trunk and the upper limbs hanging freely at the sides of the body; the symmetry of the chest; rib deformities; and the symmetry of the pelvis.
Scoliosis can be detected by placing a plumb line on the occipital protuberance or the C7 spinous process. This test can determine whether the scoliosis is balanced or not. If the lead weight starting from the C7 vertebra falls into the intervertebral fold, the scoliosis is balanced, with the C7 and S1 spinous processes aligned. If the plumb line falls outside the intervertebral fold, the scoliosis is unbalanced. The thoracic and/or lumbar curvature can be measured using a scoliometer.
Scoliosis can be detected by placing a plumb line on the occipital protuberance or the C7 spinous process. This test can determine whether the scoliosis is balanced or not. If the lead weight starting from the C7 vertebra falls into the intervertebral fold, the scoliosis is balanced, with the C7 and S1 spinous processes aligned. If the plumb line falls outside the intervertebral fold, the scoliosis is unbalanced. The thoracic and/or lumbar curvature can be measured using a scoliometer.
With regard to the treatment of idiopathic scoliosis, there are three therapeutic approaches: physical therapy, orthopedic treatment with braces, or surgical treatment. Physical therapy is an integral part of all treatment programs, whether used alone in cases of non-progressive scoliosis with a Cobb angle of less than 30°, or in conjunction with orthopedic or surgical treatment. Orthopedic treatment is indicated for scoliosis exceeding 30° in patients with skeletal immaturity, or for scoliosis around 20° that is progressive (worsening by 6° between two follow-up examinations conducted 6 months apart). Surgical treatment is indicated for cases in which the Cobb angle exceeds 40–45°.
The treatment plan must be tailored to each individual case, taking into account not only the specific medical circumstances but also the family’s circumstances and the feasibility of adhering to the treatment regimen. It must be continuously adjusted based on the results obtained; therefore, medical checkups are required every 6 months throughout the growth period, and annually after skeletal maturity is reached.
The progression of scoliosis without treatment depends on its severity and type, but in general it can lead to a progressive worsening of the spinal curvature, especially during periods of rapid growth, such as puberty. Without intervention, scoliosis can have the following consequences: progressive increase in the angle of curvature, chronic pain, noticeable body asymmetries, pulmonary and cardiovascular complications, limited spinal mobility, and a negative impact on quality of life.
For the early diagnosis of scoliosis, it is essential that every parent carefully observe their child’s back and recognize the characteristics of this condition, that all children be examined periodically by their family doctor and/or school physician, and that screening programs be implemented for early detection. If scoliosis is suspected, a consultation with a specialist is required, during which the diagnosis is established based on a clinical examination and diagnostic tests, after which an appropriate treatment will be recommended.
Bibliography
1. Iconia Borza – Patologia aparatului locomotor – noțiuni de ortopedie și traumatologie, Editura Mirton, Timișoara, 2006
2. Dinu M. Antonescu – Patologia aparatului locomotor, vol II, Editura Medicală, București, 2005-2008